On March 13, 2026, a groundbreaking conference took place in Zurich, addressing one of the most complex questions of our time:
How are neurobiological diversity and the development of gender identity connected in children and adolescents?
Under the title “Who am I?”, experts from medicine, psychology, and education explored the intersections of two spectra that are becoming increasingly relevant both in clinical practice and in everyday life.
Neurodiversity: Diversity instead of disorder
The term neurodiversity describes the natural variation in human brain development. Neurodivergent individuals — including those on the autism spectrum, with ADHD, dyslexia, or giftedness — process information differently from what is considered the societal “norm.”
A central focus of the conference was depathologization. The label “neurodivergent” is intended to relieve those affected:
moving away from a purely disorder-based perspective toward the acceptance of neurological traits that are often invisible from the outside, yet profoundly shape perception and social interaction.
Gender identity in transition
Alongside neurobiological diversity, our understanding of gender has evolved.
Gender is a spectrum.
Where categories such as “homosexual” or “transsexual” were once rigidly defined, today’s adolescents often actively and individually define their identities — for example as genderqueer, non-binary, or asexual.
Important points to understand:
- Gender identity (the internal sense of who one is) cannot be determined from the outside.
- Most people develop gender constancy early on, but during adolescence, fluctuations and identification within the non-binary spectrum increase.
- Non-binary individuals do not, or only partially, identify with the categories “male” or “female.”
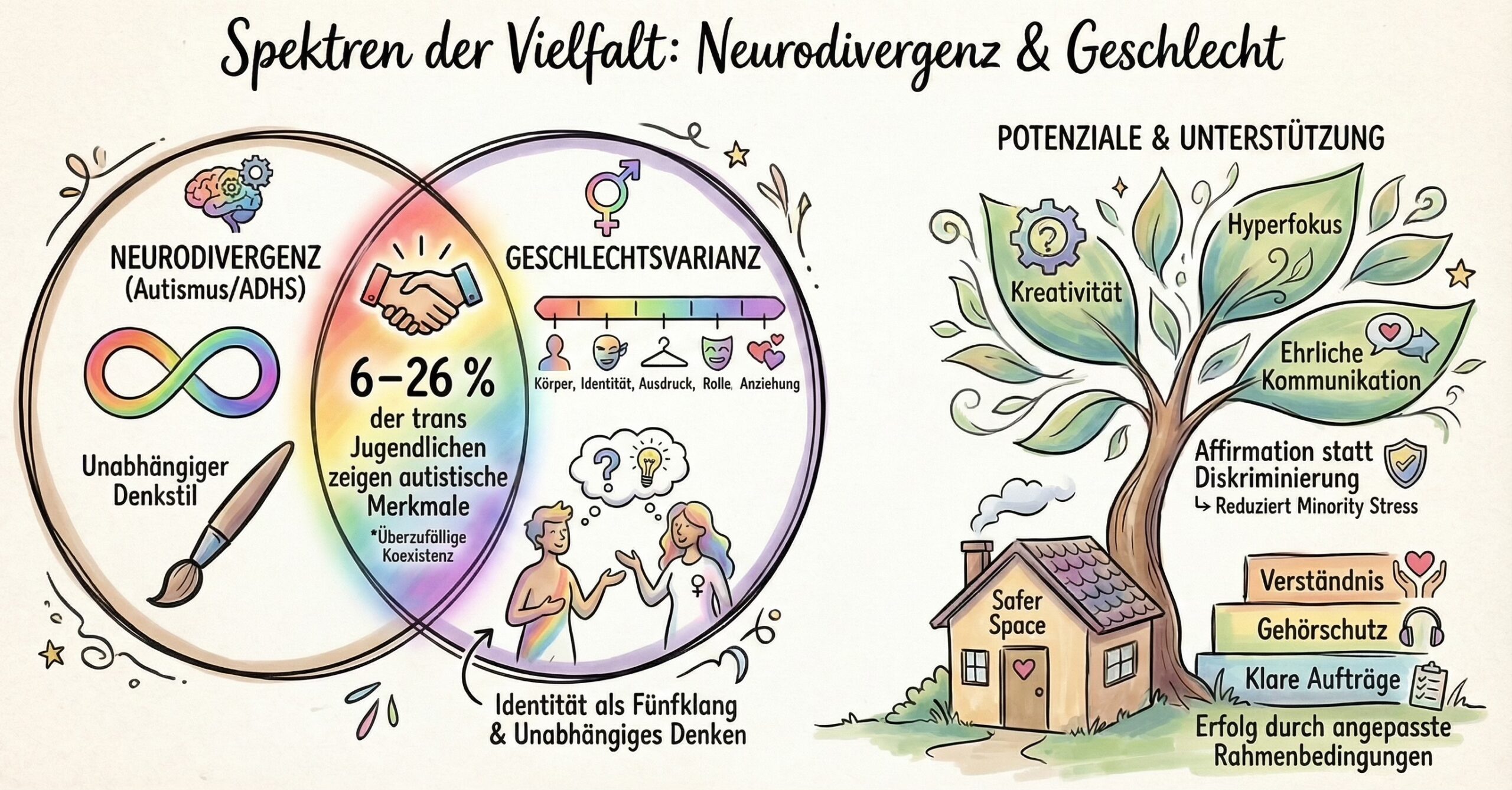
When the spectra meet: The intersection
A key focus of the conference was the above-average co-occurrence of neurodivergence and gender diversity.
Studies show that around 9% to 11% of adolescents in gender clinics have an autism diagnosis — a multiple compared to the general population.
Why is this the case? Several explanatory models were discussed:
- Cognitive style: Autistic individuals often rely less on social norms and may therefore question gender roles more critically.
- Shared vulnerability: There may be overlapping genetic or neurobiological factors.
- Minority stress: The interaction of neurodivergence and social exclusion may intensify identity-related distress.
Specific challenges and protective factors
Young people at this intersection often experience double minority stress.
The risk of psychological distress, anxiety disorders, and suicidality is alarmingly high.
50–70% of trans adolescents report suicidal thoughts or self-harm.
Key protective factors identified include:
- strong support from family and peers
- social transition (living in one’s affirmed gender)
What is needed in support and care?
For professionals and parents, the conference provided clear recommendations for a sensitive approach:
- Open-ended attitude: Support does not mean steering in a specific direction, but validating the identity exploration process and allowing time.
- Adapted communication: Especially for autistic adolescents, clear structures, reduced sensory input, and visual aids are crucial.
- Inclusive language: Using a person’s chosen name and pronouns is an act of respect and safety.
- Validation instead of skepticism: Parents’ concerns should be taken seriously — without invalidating the child’s identity.
Conclusion
Neurodiversity and gender diversity are not “trends” or “diagnostic fads,” but expressions of human diversity.
The conference made one thing clear:
We need to learn to look beyond binary norms.
By adapting our frameworks and focusing on strengths, we can create opportunities for success and help young people find their place in society — exactly as they are.
Sources
The following sources formed the basis of this blog post on the conference:
- Dr. med. univ. Cornelia Galanda: Neurodivergenz im Kindes- und Jugendalter mit Fokus auf Autismus und ADHS. Stiftung visoparents.
- KD Dr. med. Dagmar Pauli: Trans, nicht-binär, gender-nonconforming. Was brauchen genderdiverse Kinder und Jugendliche aus medizinisch-therapeutischer Perspektive? Psychiatrische Universitätsklinik Zürich / Stiftung visoparents.
- Evianne Hübscher: Geschlechtervielfalt – Nonbinarität: Die vielfältigen Dimensionen von Geschlecht. Geschlechter-Radar / Stiftung visoparents.
- Tanja Schenker: Wenn Neurodivergenz und Geschlechtsvarianz zusammentreffen. Psychiatrische Universitätsklinik Zürich / Stiftung visoparents.
These materials also include numerous references to international studies (e.g., Warrier et al., 2020; de Vries et al., 2014) as well as medical classification systems such as ICD-11 and DSM-5, which form the scientific foundation of the conference.